

Introduction
Pediatric-onset Evans syndrome (pES) is defined by the association between immune thrombocytopenic purpura (ITP) and autoimmune hemolytic anemia (AIHA) before the age of 18 years and may be associated to various immunopathological manifestations (IMs). No comprehensive study of this rare disease exists, and its long-term outcomes are poorly described.
Methods
Patients from the nationwide French prospective OBS'CEREVANCE cohort with pES and more than 5 years of follow-up were included (excepted pES secondary to bone marrow transplantation or primary immunodeficiencies known at the inclusion). All patients, including those with less than 5 years of follow-up, were included in survival analyses. Multivariate Cox proportional hazards model was used to analyze factors associated with time-dependent variables.
Results
Of the 216 patients with pES in the cohort, 151 (88 males and 63 females) were included with a median (min-max) follow-up time after first cytopenia diagnosis of 11.3 (5.1-38) years. Median age at final follow-up was 18.5 (6.8-50.0) years.
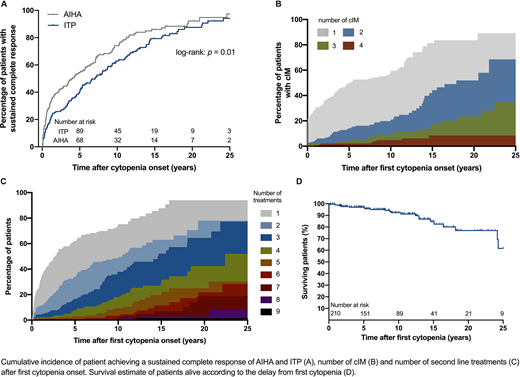
The proportion of patients achieving a sustained complete response (i.e. persisting until final follow-up) increased after cytopenia onset (Fig. 1A). ITP and AIHA were in complete remission in 40.5% and 54.5%, 74.1% and 62.3%, and 78.4% and 86% of patients at 5, 10, and 15 years, respectively.
Clinical IMs (cIMs) developed in 100/151 patients (66%), before the first diagnosis of cytopenia in 21/100 cases. The number of cIMs increased over time (Fig. 1B). The proportions of patients with one and more than one cIM were 50% and 14%, 57% and 19%, and 81% and 44% at 5, 10, and 15 years after the first cytopenia diagnosis, respectively. A broad spectrum of cIMs were present, lymphoproliferation (n = 71), dermatological (n = 26), gastrointestinal/hepatic (n = 23), and pneumological manifestations (n = 16) being the most common. Three patients had a hematological malignancy. Biological IMs (bIMs) were diagnosed in 101/151 patients (67%) and also increased over time, with hypogammaglobulinemia (n = 54) being the most common. Autoimmune neutropenia developed in 43 patients (28.5%) and was independently associated with the number of cIMs (hazard ratio [HR], 2.4; 95% confidence interval [CI], 1.5-3.8; p = 0.0002). Severe or recurrent infections were present in 53 patients (35%).
The number of second-line treatments received (i.e. other than steroids and immunoglobulins) increased over time without reaching a plateau (Fig. 1C). Half of the patients had received at least one, two, and three different treatments at 2.7, 10.5, and 14.7 years after the first cytopenia diagnosis, respectively. The number of cIMs was independently associated with the number of second-line treatments received (HR, 1.3; 95% CI, 1.08-1.6; p = 0.006).
Systemic lupus erythematosus (SLE) was diagnosed in 11/151 patients (7.3%, 1/88 males and 10/63 females) and autoimmune lymphoproliferative syndrome (ALPS) in six (4.0%).
Sixteen of the 151 patients followed for more than 5 years (10.6%) died, and seven died before the fifth year of follow-up (23 deaths in total). Survival at 5, 10, and 15 years after the first cytopenia was 97%, 92%, and 84%, respectively (Fig. 1D). Deaths occurred regularly throughout the follow-up period, at a median age of 18.0 (1.7-31.5) years. The most frequent cause of death was infections (n = 12, 52%). Four patients (18%) died of hemorrhage, all were less than 13 years old. The numbers of second-line treatments (HR, 1.3; 95% CI, 1.1-1.6; p = 0.004) and severe or recurrent infections (HR, 3.4; 95% CI, 1.2-9.7; p = 0.02) were independently associated with mortality after 5 years of follow-up.
Overall, 20-year-old compared to 10-year-old patients more frequently showed a sustained complete response for AIHA (72% vs. 30%) and ITP (50% vs. 26%), but more frequently had cIMs (74% vs. 37%), bIMs (75% vs. 39%), and ongoing second-line treatments (88% vs. 47%; p < 0.001 for all comparisons).
Conclusions
Long-term outcomes of pES were associated to IMs and second-line treatment burden, not active cytopenia. The significant mortality rates, mostly among adolescents and young adults, were linked to drug-induced and/or constitutive immunodeficiencies. Few cases were associated with SLE or ALPS, which is consistent with a heterogeneous genetic background. These results highlight the importance of multidisciplinary care during the transition from childhood to adulthood.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal